
Research Article | DOI: https://doi.org/10.31579/2578-8868/037
1Professor & HOD, Department of Neurology, Narayana Medical College and Hospital, India
2Department of Neurology, Narayana Medical College and Hospital, India
3Department of Neurology, Narayana Medical College and Hospital, India
4Department of Management Information System, Narayana Medical College and Hospital, India
*Corresponding Author: NS Sampath kumar*, Sangamithra Gandra, Prasad PNS , Venkata Ramya Bola, Professor & HOD, Department of Neurology, Narayana Medical College, Chinthareddypalem, Nellore , Andhra Pradesh, India.
Citation: N S Sampath kumar ,Overview of Intracerebral Hemorrhage J Neuroscience and Neurological Surgery. 2(1);DOI:10.31579/2578-8868/037
Copyright: © 2018 Dr. N S Sampath kumar, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 January 2018 | Accepted: 27 January 2018 | Published: 31 January 2018
Keywords: stroke; intra cerebral hemorrhage; hypertension
Stroke is categorized into two major subtypes i.e., ischemic and hemorrhagic and is one of the major causes of morbidity and mortality worldwide. Primary intracerebral hemorrhage (ICH), i.e. spontaneous extravasation of blood into the brain parenchyma, begins very suddenly and is a medical catastrophe. The well-known risk factors for ICH are hypertension, heavy drinking of alcohol, and anticoagulant medication. Risk factors for early death include clinical and radiological severity of the bleeding. Moreover, intraventricular bleeding, use of anticoagulants, and high blood pressure on admission also predict early death after ICH. CT brain imaging is the immediate modality for establishing diagnosis and supplemented with MR imaging depending upon aetiology. Treatment of patients with ICH includes standard supportive care, medical management and surgical intervention.
Stroke is categorized into two major subtypes i.e., ischemic and hemorrhagic and is one of the major causes of morbidity and mortality worldwide [1]. Primary intracerebral hemorrhage (ICH), is defined as bleeding that evolves within the tissue of the brain. It results from the rupture of small, penetrating vessels and is usually attributed to hypertension or amyloid angiopathy. After the onset, bleeding may continue and the hematoma grow for several hours, leading to progressive clinical deterioration of the patient’s condition [2-4]. Computed tomography (CT) soon after the onset of symptoms is crucial for the diagnosis. Case fatality is high, as 35–52% of patients die within 30 days and half of the deaths occur in the first two days [5-7]. Up to 58% of survivors have been reported to be functionally independent at 1 year [8]. The incidence of ICH varies geographically, ranging from 10 to 20/100,000 persons per year [9,10]. ICH incidence in Finland seems to be somewhat higher, 21 to 31/100,000 persons/year [11-13]. The highest incidence has been reported in Japan, 48/100,000 persons/year. The well-known risk factors for ICH are hypertension, heavy drinking of alcohol, and anticoagulant medication [14,15]. Risk factors for early death include clinical and radiological severity of the bleeding. Low Glasgow Coma Scale (GCS) score (i.e. level of consciousness) and hematoma volume appear to be the most important predictors for early death after ICH [16]. Moreover, intraventricular bleeding, use of anticoagulants, and high blood pressure on admission also predict early death after ICH [5, 8, 14 and 17-19]. Treatment of patients with ICH has turned out to be complicated in many ways.
The clinical presentation of ICH usually starts with a focal neurological deficit followed by progression of symptoms over minutes to hours [20]. This symptomatic progression over hours is uncommon in patients with ischemic stroke. Another manifestation is a sudden decline in the level of consciousness. Increased blood pressure and impaired level of consciousness are common. Vomiting is more common in patients with ICH. Headache is more common with ICH than with ischemic stroke but less common than with subarachnoid hemorrhage [21]. Diagnosis is confirmed by brain imaging. Computed tomography (CT) and magnetic resonance imaging (MRI) show the presence of ICH equally well. CT has the advantage of demonstrating the intraventricular extension of the hemorrhage, while MRI shows better the underlying structures and perihematomal edema.
B. Subgroups of intracerebral hemorrhage
1. Primary intracerebral haemorrhage
The term ‘spontaneous intracerebral hematoma’ refers to non-traumatic bleeding
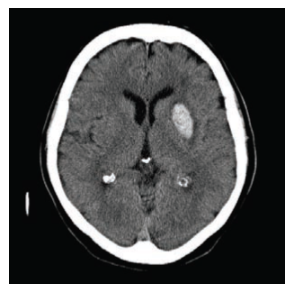
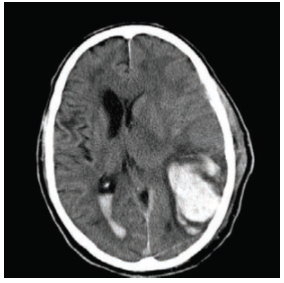
into the brain parenchyma [1]. ‘Primary intracerebral hemorrhage’ means a spontaneous hematoma without any secondary cause, such as vascular abnormality or brain tumour, which have been ruled out by radiological or pathological investigations [14]. Primary intracerebral hemorrhage originates from bleeding of small arteries damaged by chronic hypertension, cerebral amyloid angiopathy (CAA), or other causative factors [14,22]. Almost two thirds of primary intracerebral hematomas are related to chronic hypertension [23]. In these cases the hematoma is typically located deep, in the basal ganglia, thalamus, or brain stem [1] figure 1. ICHs related to CAA, on the other hand, are mainly lobar or subcortical hematomas [22] Figure 2
2. Secondary intracerebral haemorrhage.
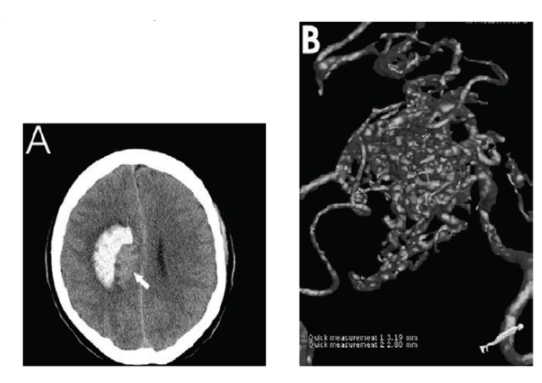
Only 12–18% of all ICH cases are classifiable as the secondary type of ICH [14]. The most important causes of secondary ICH are vascular abnormalities, which carry the risk of rebleeding. The secondary causes of ICH are represented in table 1.
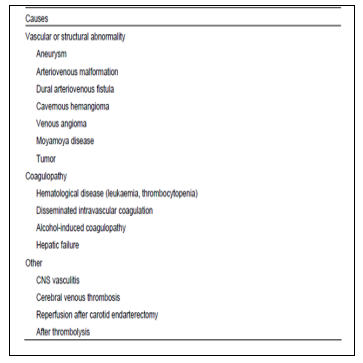
Source: Predictors of early deterioration and mortality in black Americans with spontaneous intracerebral hemorrhage. Stroke (1995) 26: 1764–1767.
C. Risk factors of primary intracerebral hemorrhage
1. Untreated and treated hypertension
Hypertension is the most prevalent risk factor for ICH [23]. It is considered a major risk factor in half of all patients presenting with ICH and in 75% of those with deep hematomas [12,24-30]. The risk of ICH increases at higher blood pressure values [31]. Untreated hypertension has been found to be a highly prevalent risk factor for hemorrhagic stroke (ICH and subarachnoid hemorrhage combined) [29, 32].
2. Diabetes
Diabetes is a well-known risk factor for ischemic stroke [33, 34]. On the other hand, it is less clear whether there is an association between diabetes and ICH [35].
3.Amyloid angiopathy and genetic factors
Cerebral amyloid angiopathy (CAA) is a major cause of lobar ICH in older patients [14, 36]. CAA is a degenerative process of arterial media, which mainly affects cortical and leptomeningeal vessels, predisposing to ICH. CAA is caused by the deposition of β-amyloid protein on the vessel wall [14]. The prevalence of CAA rises with age, being approximately 60% among those over 90 years of age [36]. The diagnosis is clinically suspected in multiple lobar bleedings with no other obvious cause of ICH in patients 55 years of age or older [37].
4. Alcohol consumption and stimulant use
The relationship between alcohol intake and increased ICH risk has been identified in many case-control studies [26&38-43]. Short-term recent moderate or heavy binge alcohol intake within 24 hours or one week seems to be a more important risk factor for ICH than long-term habitual heavy drinking [26]. Amphetamine or cocaine use can provoke ICH. This uncommon etiology is mainly seen in young adult [44]. Cigarette smoking is a well-known predictor of ischemic stroke in both men and women, [45, 46]. but its role as a risk factor for ICH is less clear.
5. Use of anticoagulants and platelet inhibitors
The risk for ICH in warfarin users has been reported to be 8 to 10-fold compared with nonusers [47, 48]. ICHs associated with oral anticoagulation account for a considerable proportion of all ICHs (6.9
1. Conservative treatment
Conservative treatment of ICH covers all emergency and critical care procedures except operative treatment. In general, all patients with ICH should be admitted to a neurosurgical or neurological intensive care setting, because it reduces mortality [69].
2. Securing the airways
The onset of ICH is typically followed by a rapid decline of consciousness and progression of neurological symptoms. Loss of the normal reflexes to maintain an open airway develops, which increases the risk of aspiration, hypoxemia, and hypercapnia [72]. Sedatives (such as propofol) and non-depolarizing neuromuscular drugs (such as vecuronium) are used to facilitate the intubation procedure.
3. Controlling blood pressure
High admission MABP has been repeatedly reported to predict early death and poor outcome after ICH [60,62]. Blood pressure maintains the cerebral perfusion pressure (CPP), and overaggressive lowering of blood pressure may theoretically worsen cerebral perfusion in cases with high intracranial pressure (CPP = MABPICP). The recommendations of the European Stroke Initiative 2006 [15] and the American Stroke Association 2007 [73] for the management of high blood pressure are presented in Table 3.
The recommended medication for hypertension consists of intravenous 10 to 80 mg boluses of labetalol at every 10 minutes [74].
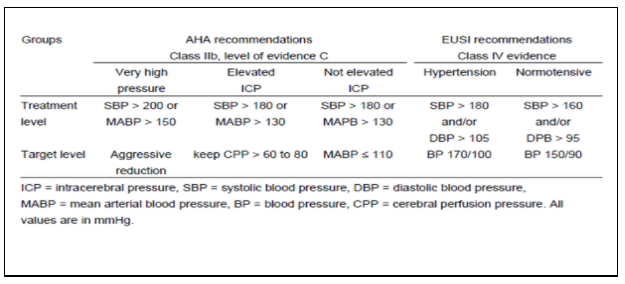
Source: The recommendations of the European Stroke Initiative 2006 (Steiner et al. 2006b) and the American Stroke Association 2007 (Broderick et al. 2007) for the management of high blood pressure.
4. Management of increased intracranial pressure
Emergency management of elevated intracranial pressure (ICP) includes head elevation, use of mannitol, and hyperventilation even before the installation of any ICP measurement devices. The management also includes sedation, phenobarbital therapy, hypothermia, and fluid infusion according to the cerebral perfusion pressure (CPP) guided therapy [50, 75-77]. Neurosurgical methods for lowering ICP include placement of an external ventricular catheter and decompressive craniectomy [78].
5. Reversal of anticoagulation
Anticoagulant treatment preceding the onset of ICH is related to high mortality and poor functional outcome compared to ICH without preceding anticoagulation [25,49,79]. Anticoagulation should be reversed immediately to prevent further deterioration, and warfarin users should have their International Normalized ratio (INR) value lowered below 1.4 immediately after the diagnosis of ICH [80]. This is done by using either fresh frozen plasma or prothrombin complex concentrate together with vitamin K. If the patient has used heparin or low molecular weight heparins (LMWH) before the onset of ICH, the effect of the medication should be reversed with protamine sulphate [81].
Conclusion
ICH is most commonly caused by hypertension, arteriovenous malformations, or head trauma. Intracerebral hemorrhage results in sudden, severe symptoms like headache, loss of consciousness, vomiting but headache may be absent (particularly in the elderly), and small hemorrhages may mimic ischemic stroke. CT brain imaging is the immediate modality for establishing diagnosis and supplemented with MR imaging depending upon aetiology. Treatment of patients with ICH includes standard supportive care, medical management and surgical intervention.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
